Annals of Neurosciences, Vol 16, No 2 (2009)
Annals of Neurosciences, Volume 16, Number 2, April 2009
Dissemination of tubercular bacilli by shunt placement
Corresponding Author
Sandeep Mohindra
E-mail : satya_sandee@yahoo.com
Phone: 0172-2756699, 09815535675
Fax:0172-2744401
ABSTRACT
A unique case of tubercular meningitis, developing shunt complication is being reported. We present a pediatric patient with tubercular ulcer formation at abdominal shunt insertion site, marking a grotesque form of tuberculosis. The final outcome of the child was satisfactory after complete course of chemotherapy.
KEYWORDS : Trigeminal autonomic cephalgias, Headache, Hypnic.
doi: 10.5214/ans.0972.7531.2009.160211
Introduction
The widespread prevalence of tubercular meningitis among Afro-Asian population continues to indicate the socio-economic disparity between Eastern and Western parts of world. Eighty percent of tubercular meningitis develops hydrocephalus, of which 65% require CSF diversion procedure1. At our institution, 1004 patients with tubercular meningitis have undergone CSF diversion surgery in the last one-decade. Two-third of patients belongs to pediatric age group and twice is males. We present a unique case of tubercular meningitis, which had dissemination of tubercular bacilli along the shunt, even while on anti-tubercular chemotherapy.
Case Report
A 3-year-old female presented with altered sensorium and low-grade fever of 6 months’ duration. After investigating with CT scan of head and chest radiograph, the child was diagnosed to have miliary tuberculosis, tubercular meningitis and consequent hydrocephalus (figure 1). The child was started on anti-tubercular chemotherapy, consisting of 4-drugs(lsoniazid, Rifampicin, Pyrazinamide, Ethambutol) and a ventriculo-peritoneal shunt was placed. The CSF culture taken during shunt insertion was positive for tubercular bacilli after 6 weeks of incubation. After remaining asymptomatic for 1 year, the child complained of fluctuant swelling all along the shunt tract, with no evidence of acute inflammation. When lower end of shunt was exteriorized, the pus drained grew acid fast bacilli and the wound margins of abdominal wall when biopsied also confirmed the granulomatous inflammation, consistent with tubercular wound or ulcer. The abdominal shunt wound gave way and the pus got evacuated, leaving a typical punched out tubercular ulcer (figure 2). Ultrasonography showed parietal wall pus collections, with echogenic debris. CT scan of upper abdomen revealed pus pocket with in parietal wall of upper abdomen (figure 3). The whole shunt assembly was removed and the patient continued on anti-tubercular therapy. At 6 months of follow-up, the child is asymptomatic with completely healed ulcer. The child did not require cerebrospinal fluid diversion procedure at follow-up.
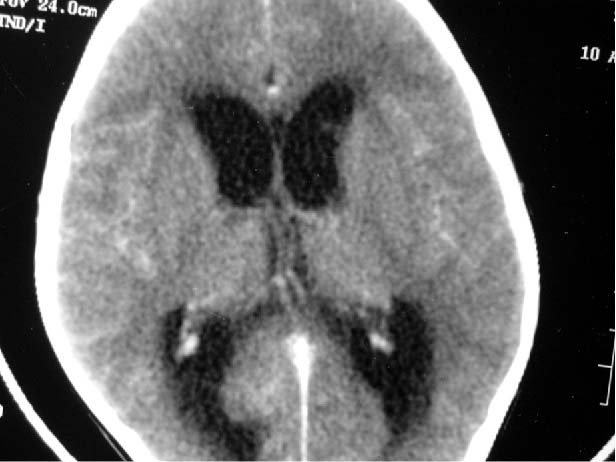
Figure 1 : Axial section of contrast CT scan of head showing tubercular hydrocephalus.
Discussion
The tubercular bacilli positivity is 30% in tubercular meningitis2. Our case had miliary tuberculosis, hydrocephalus, mediastinal adenopathy, as well as tubercular bacilli positivity. The extracranial dissemination of tubercular bacilli from ventricular CSF, occurred through shunt tract. A fatal case of tubercular bacilli dissemination through ventriculo-atrial shunt, causing recurrent miliary tuberculosis has been reported earlier3. Hence, the prosthesis induced bacilli transmission and spread has been documented earlier. However, the persistence of bacilli after one year of chemotherapy is noteworthy. The alternate explanation is the spillage of tubercular node content into the shunt tract, making a subcutaneous cold abscess.
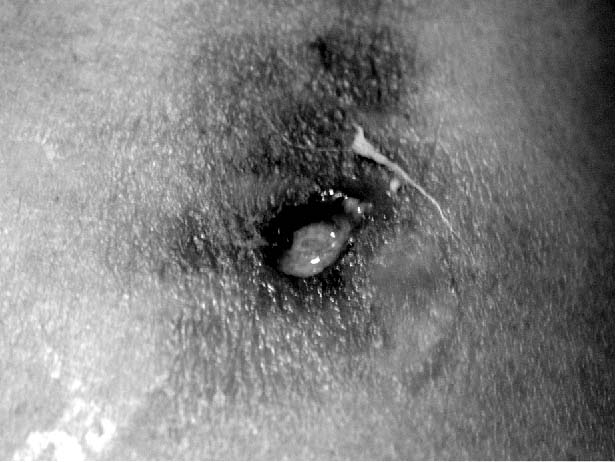
Figure 2 : Clinical photograph of abdominal wound of shunt placement, showing a typical tubercular ulcer. The ulcer is typically punched out, with vertical walls, without any signs of inflammation.

Figure 3 ; Axial section of abdominal CT scan showing a pus collection with in parietal wall, a cold abscess.
After initiating chemotherapy, the time taken to sterilize the ventricular CSF is usually 2 weeks, while it takes 4 weeks to sterilize the lymph nodes1. The persistence of bacilli for such a prolonged duration makes the present case exceptional1.
We propose that a minimum of 2 weeks should lapse before inserting the shunt, so as to avoid such a complication. The gold standard of management remains full dose chemotherapy for prolonged duration of 12-18 months1.
Conclusion
Tubercular bacilli may persist, in spite of full dose of chemotherapy. A latent period of 2 weeks may be provided, before inserting shunt, so as to minimize the chance of bacilli dissemination.
Competing interests - None, Source of Funding - None
Received Date : 7 April 2009; Revised Date : 29 April 2009
Accepted Date : 9 May 2009
References
1. Van den Bos F, Terken M, Ypma L, et al. Tuberculous meningitis and miliary tuberculosis in young children. Trop Med Int Health 2004; 9:309-313.
2. Thwaites GE, Hien T T. Tuberculous meningitis ; many questions, too few answers. Lancet Neurology 2005; 4 : 160-170.
3. Shibolet S, Dan M, Jedwab M, et al. Recurrent miliary tuberculosis secondary to infected ventriculoatrial shunt. Chest 1979; 76 :328-330.
(c) Annals of Neurosciences.All Rights Reserved