Annals of Neurosciences, Vol 17, No 3 (2010)
Annals of Neurosciences, Volume 17, Number 3, July 2010
Altered sensorium and multiple cranial nerve palsies in a recently diagnosed diabetic
Corresponding Author |
ABSTRACTWe report a recent diabetic who presented with hyperglycemic, hyperosmolar, non ketotic state with coma and multiple cranial nerve palsies due to an associated previously undetected sinus infection. This is a classic case revisited purely for its educational value in terms of clinical photographs, tissue biopsy and imaging findings. These findings reiterate the devastating neurological consequences of fungal sinusitis in diabetic patients. KEYWORDS: Diabetes, Hyperglycemic Hyperosmolar Non Ketotic State HHNS, sinusitis, mucormycosis doi: 10.5214/ans.0972-7531.1017312 |
Introduction
Diabetic patients are prone to infections. Certain rare infections like rhinocerebral mucormycosis, emphysematous infections of gall bladders urinary tract & malignant or invasive otits externa are seen exclusively in diabetic populations.1
These infections must be particularly sought in patients presenting with in Hyperglycemic Hyperosmolar Non-ketotic State (HHNS).1 We present here a case report of an elderly diabetic male who ran a downhill course after harboring a rare fatal infection.
Case report
A 56 years old male, recently detected diabetic was hospitalized in medical ward in a profoundly dehydrated state and altered mental status.
He had leucocytosis [TLC-24,000/cumm], high blood sugars [480 mg/dl] and renal insufficiency [Blood Urea 99.0 mg/dl, Sr. Creatinine 1.9 mg/dl]. His serum sodium was 138.3 MEq, serum potassium was 4.7 MEq and his calculated osmolality was 347.9 MEq/lt (Normal 280-290 MEq/lt). His blood pH was 7.337. ECG, X-Ray chest, Sr. Lipids, Fundus Examination done on admission, was normal.
He was diagnosed to be in Hyperglycemic Hyperosmolar Nonketotic State HHNS with renal insufficiency and septicemia and treated for HHNS with fluids and intravenous insulin and parenteral antibacterials. Within 48 hours, he became well hydrated and sensorium returned to normal as evaluated on regular rounds. Sugars were well controlled.
His renal function tests were normal (urea 30.6, creatinine 0.9) and leucocytosis subsided with total leucocyte count returning to a normal of 7,400. Blood cultures were sterile. But 3 days later, patient complained of pain in the right eye and right maxillary region. He also developed complete ptosis, covering the pupillary area (Fig 1).
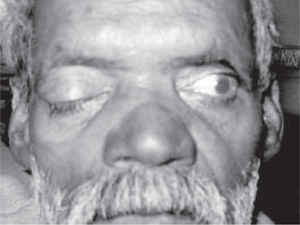
Fig. 1: Significant Ptosis
His sensorium had also again deteriorated with disorientation to time place and person. On examination, there was no vision in the right eye which apart from ptosis also revealed restricted ocular movements suggestive of III, IV and VI cranial nerve palsies. However, there was no chemosis or redness in the eyes.
There was no Pupillary reflex sparing which is typical of diabetic III nerve occulopathy. Corneal reflex in the right eye was absent. Papilledema was present by now.
There was suspicion of orbital apex involvement and C.T. scan of orbit and brain was ordered. C.T. scan revealed normal brain anatomy but right optic neuritis and orbital myositis was noted. Nasal septum was deviated towards right side with right maxillary sinusitis and mucosal hypertrophy forming polyp between nasal septum and middle turbinate. There was evidence of involvement of ethmoid and sphenoid sinuses on the right side. There was a granuloma at right orbital apex. Some destruction of contiguous bone was also reported (fig 2).

Fig. 2
ENT consultation revealed black necrotic mass in right nasal cavity and mild right facial swelling. The mass was sent for examination and empirically I.V. Amphotericin B (conventional) was started in standard doses.
Patient was taken for emergency surgery by ENT service and debridement of necrotic mass was done. All black pieces including necrosed inferior and middle turbinate were excised.
There was a mass in anterior ethmoid air cell which was cleared. There were mucosal polyps in right nasal cavity which were removed. There was septal perforation.
Tissue was sent for culture and biopsy. Immediate report on 10% KOH mount was done. It showed characteristic broad, non-septate, ribbon-like hyphae with wide-angled branching. Ptwas given second dose of conventional amphotericin B (1.5 ml / Kg) and was kept on insulin infusion, but post-operatively he could not regain consciousness and succumbed to his illness within a very short span.
Later, fungal culture grew mucormycosis. Microscopic characterization of the fungal isolate was carried out and a rapid, white, fluffy growth was observed after 24 h on SDA without cycloheximide, incubated at 25°C and 37 °C.
On staining with Lacto-phenol cotton blue(LPCB), wide, hyaline, aseptate hyphae were seen. Sporangiophores, smooth-walled, non-septate, were seen originating singly or in groups from stolons directly above the rhizoidal tufts. Collapsed columella resembling umbrella which differentiate from other zygomycetes were seen (fig 3).
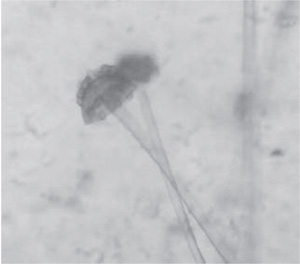
Fig. 3
Final impression Hyperglycemic Hyperosmolar Non-ketotic State with Rhino-cerebral mucomycosis.
Discussion
Mucormycosis is a serious entity which usually affects patients with DKA/ HHNS. Fungi from order mucorales, commonly found in environment, usually non pathogenic, likely to be inhaled daily by normal individuals but creating catastrophe in immunocompromised settings are the etiologic agents for mucormycosis.
They have broad ribbon like non septate hyphae, 10-20microns with branches at right angles .In diabetic patients especially with elevated blood sugars and acidemia, spores germinate and hyphae develop. Fungi begin an inexorable march invading blood vessels and surrounding tissues.
As blood vessels become involved, thrombosis occurs; tissue necrosis results and fungi continue to grow in devitalized tissue.1 In Orbital apex syndrome there is severe unilateral visual loss and opthalmoplegia with minimal orbital inflammation. It is usually caused by posterior ethmoid/sphenoid sinusitis. Sinuses are adjacent to orbital apex through which runs the optic nerve, Cranial nerves III, IV, VI and first division of V.2
Most cases with associate diabetes may be attributed to mucormycosis. Usual Cause of blindness is thombosis of retinal artery by mucormycosis. Most patients die because of carotid artery thrombosis/cavernous sinus thrombosis.
The three factors which influence outcome are reversal of underlying condition, aggressive surgical debridement and antifungal therapy, hence treatment involves extensive debridement, good sugar control, I/V amphotericin B. A series of patients of acute sinusitis with neuro-ophthalmic complications have been previously reported from our institute.3
In summary our patient described above was an uncontrolled neglected diabetic who inhaled mucor, developed mucormycosis, had sinusitis which progressed to involve the orbital apex and further continued to run its inexorable march only to prove fatal despite our best efforts.
Competing interests- None, Source of Funding - None
Received Date : 8 June 2010; Revised Date : 24 July 2010
Accepted Date : 3 August 2010
References
1. Sugar AM, Mucormycosis. (Eds) Fauci A, Braunwald S, Harrison’s Principles f Internal Medicine, NY, The Mc Graw Hill Companies 2008;1261-62.
2. Yeh and Foroozan. Orbital apex syndrome. Current Opinion in Ophthalmology 2004;15:490-498.
3. Gupta S, Goyal R. Neuro-ophthalmic complications of acute paranasal sinusitis a surgical emergency. Annals of Neurosciences 2010;16(3):123-124.
(c) Annals of Neurosciences.All Rights Reserved