Annals of Neurosciences, Vol 18, No 1 (2011)
Annals of Neurosciences, Volume 18, Issue 1 (January), 2011
Systemic infection and inflammation as trigger factors of ischemic stroke
KEY WORDS
Infection
High sensitivity CRP
Cerebral infarction
Risk factors
Stroke triggers
ABSTRACT
Background: Chronic risk factors are well understood in cases of stroke as well as myocardial infarction. Till date, several triggers for stroke are still under evaluation. Researchers have previously evaluated the relationship between preceding infection and inflammation and stroke onset. Purpose: The purpose of study is to define the stroke triggers in a better way and to provide little more information for early intervention by controlling infections or other trigger factors Methods: In this retrospective study, a standardized questionnaire was carried out to evaluate the signs, symptoms of preceding (<14 days) infection, physical/mental health, drug history, TIA etc. of 70 ischemic stroke patients and 80 non-stroke out-patient department patients as control groups. Important biochemical tests e.g. high sensitivity CRP, leukocytes count, blood sugar, lipid profile, etc. were also taken into consideration. Recent (15 days) prior infection, mainly respiratory tract infection and urinary tract infection, which were likely to be important stroke triggers, were compared between the ischemic stroke groups and the non-stroke patients (control group). Results: It was found that respiratory tract infection is the most common type of infection (48.5%) compared with the non-stroke control group (30%). Apart from this, there were clinical evidence of infections like gastroenteritis, RTI, UTI etc which were biochemically established by leukocytosis and increased high-sensitivity C-Reactive Protein levels, well-known early diagnostic tools that have good predictive value. This study reveals that well-controlled diabetic, hypertensive or non-diabetic normotensive patients can suddenly develop ischemic stroke following recent infection as evidenced by clinical features, increased levels of high-sensitivity CRP and leukocytosis. Conclusion: These diagnostic tools implicate the value of early treatment of febrile illness and introduction or adjustment of doses of antiplatelet agents, antibiotics, etc. to reduce the actual stroke incidence, though it needs multicentre large community based prospective trials to evaluate stroke prone state and effective preventive measures tools at the same time.
doi : 10.5214/ans.0972.7531.1118106
Corresponding Author:
Prasanta Kumar Gangopadhyay
Tel : +91-33-24114771
E-mail : pkganguly100@yahoo.com
Introduction
Stroke is the second most leading etiology of death all over the world.1 Cerebral infarction of ‘unknown etiology’ represents about 40% of cases in the stroke data bank and the importance of potential precipitants has not been well documented.2 Chronic risk factors and some markers are now fairly well understood e.g. age, sex, race, obesity, hypertension, diabetes, dyslipidemia, smoking etc. Some patients with multiple chronic risk factors do not know when stroke will precipitate even after perfect control or near control of these risk factors. Mittleman and others3,4 were able to show that anger and sexual activity were potential triggers of myocardial infarction. Some studies also revealed the association of myocardial infarction with prior infection and inflammatory process;5 likewise, infection appears to be an important stroke triggers.6,7,8,9,10
In the eastern parts of India this study has been done to search for the ischemic stroke triggers e.g. prior infection, physical exercise, anxiety, over eating etc. This case control study included some non-stroke minor presurgery patients and relatives of general patients without such trigger factors. Our aim is to define the stroke triggers in a better way and to provide little more information for early intervention by increasing the dose of antiplatelet drugs or by controlling infections or other trigger factors.11
Methods
We have studied seventy (70) ischemic stroke patients admitted in our hospital for acute infarct and eighty (80) age and sex matched control subjects selected randomly from the general surgery out-patient department and relatives of general patients (non-stroke cases). On the basis of a preliminary CT scan imaging of brain, hemorrhagic strokes were excluded. All ischemic stroke patients were examined thoroughly and the medical history was recorded with special emphasis on recent prior infection, fever, physical / mental stress or transient ischemic attacks besides chronic risk factors like diabetes, hypertension, obesity, smoking etc. Informed consent was obtained as per Institute Ethical Committee Guidelines, CNMC.
Exclusion criteria included valvular heart disease, congestive heart failure, renal or hepatic failure, pregnancy or any hematological disorder i.e. either thrombocytosis or thrombocytopenia, collagen vascular disease groups. Suspected alcohol addicted, immunocompromised or recently treated tuberculosis patients (<6 months of diagnosis and treatment) were also excluded.
Age and sex matched control subjects were chosen from surgery outdoors and relatives of general patients and investigations were carried out in the same way in order to compare the trigger factors in both groups. All the cases and control groups were questioned for recent febrile illness (<2 weeks) including respiratory tract infection, urinary tract infection, abscess, gastroenteritis, heavy meal / heavy exercise just before the event. Each patient underwent complete hemogram, including platelet counts, blood biochemistry including electrolytes and routine urinary analysis, highly sensitive CRP (C-reactive protein), ECG and thoracic roentgenogram, and wherever necessary, abdominal ultrasonography to exclude intra-abdominal pathology or infection. Both cases and control group of patients were asked about long term psychosocial problems; recently developed mental stress, drug abuse or quarrelling etc without any specific scale.
Results
70 ischemic stroke patients were evaluated within 1.5 ±1 days after stroke onset. Out of 70 cases, 52 were males and 18 were females. Control subjects included total number of 56 males and 24 females. Clinical and demographic features of the stroke group and control group are given in Table 1. As the study was done between May 2007 to April 2008, there was enrolment of 30 stroke cases in summer, 20 stroke cases in winter, 14 in the autumn and 6 in the rainy season (30:40) i.e. more cases were found to be around the winter and fall than in the spring and summer, which is consistent with the study report of Richard F. Macko et al.6
Up to 65% of male patients and 48.5% of all patients were smokers. 40% patients were hypertensive, 20% were diabetic and 40% were diagnosed as dyslipidemic based on the criterion of NCEP – target values.
Interestingly, it was found that most of the stroke (45.7%) occurred in the morning followed by afternoon (22.8%) and noon (17.14%) respectively, as shown in Table 2.
Though some cases occurred at late night but most of them reported at the hospital after 6 am because the incidence took place during sleep, such cases were included among early morning cases.
As this study has been done in a part of a tropical country with lower socio-economic status where there is increased prevalence of infectious diseases, so preceding infection and history of febrile illness were taken for just 2 weeks duration before stroke. Different categories of infection and stroke triggers were evaluated among seventy (70) ischemic stroke cases and compared with the eighty (80) non-stroke control subjects. The prevalence of upper respiratory tract infection and bronchitis in ischemic stroke was higher than in control subjects (48.5% versus 30%; p < 0.009). Other infections like urinary tract infections (UTI) was detected in 8.5% of the ischemic stroke patients but in none of control group (p < 0.003). Increased leukocyte counts were recorded in 34.2% of ischemic stroke patients but only in 10% of non-stroke control group. This higher rate of increased leukocyte count in stroke patients than control group (34.2% versus 10%; p < 0.0001) was most probably due to different types of infections and inflammation responsible for endothelial and platelet dysfunctions. Another area of our stroke study is estimation of highly sensitive C-Reactive Protein (hsCRP). Higher values of hsCRP were found in 40% (28/70) of stroke patients than the control subjects i.e. only 20% (16/80). This difference was due to the association of recent infections in ischemic stroke cases and it is statistically significant (p < 0.003). As the higher level of CRP may be normally found in smokers, subclinical chronic infections, atherosclerosis and inflammatory responses after brain infections but many more symptomatic febrile patients with high leukocyte count and CRP indicate correlation between recent infection and stroke occurrence. High level of CRP (>1.5mg/ dl) are present among general population who are found at risk for future first-ever myocardial infarction or stroke.12 In this study 6 patients developed ischemic strokes after heavy meal (8.5%) but none had history of heavy meal intake in the control groups (p < 0.003). 20% of the patients had history of transient ischemic attack and 20% ischemic stroke patients gave the history of heavy exercise (more in the summer season) preceding 6 hours of stroke.
Table 1: Demographic features of stroke and control groups
| Variable | Stroke Group (n = 70) |
Control Group (n = 80) |
|---|---|---|
| Age | 62.5 ± 9.55 | 61.8 ± 1.2 |
| Sex (F/M) | 18/52 | 24/56 |
| Addiction (smoking) | 34 (48.5%) | 40(50%) |
| Hypertension | 28 (40%) | 30 (37.5%) |
| Diabetes | 14 (20%) | 10(12.5%) |
| Dyslipidemia | 28 (40%) | 30 (37.5%) |
Table 2: Timing of stroke occurrences / diurnal variation
| Time | Number of cases | Percentage of cases |
|---|---|---|
| Morning | 32 | 45.7% |
| Noon | 12 | 17.14% |
| Afternoon | 16 | 22.8% |
| Evening | 6 | 8.5% |
| Night | 4 | 5.7% |
Anxiety and stress factors were detected among 14.2% of stroke patients which is a near normal value in the whole society and not higher than the control group p < 0.05. Two patients developed ischemic stroke within 2 weeks of cystostomy and cholecystectomy operative procedures. All the proposed stroke triggers involved in the onset of acute ischemic stroke are shown in the Table 3, Figure 1 and Figure 2).
Clinical and demographic features of stroke patients with recent (<2 weeks) infection and febrile illness and without recent infection as per history and clinical examination are shown in Table 4.
Table 3: Different trigger factors of stroke and control groups
| Variables | Stroke Group | Control Group |
|---|---|---|
| RTI | 34 (48.5%) | 24 (30%) |
| UTI | 6 (8.5%) | 0 (0%) |
| hSCRP | 28 (40%) | 16 (20%) |
| Leucocytosis | 24 (34.2%) | 8 (10%) |
| Exercise | 14 (20%) | 16 (20%) |
| Stress / Anxiety | 8 (11.4%) | 8 (10%) |
| Heavy meal | 6 (8.5%) | 0 (0%) |
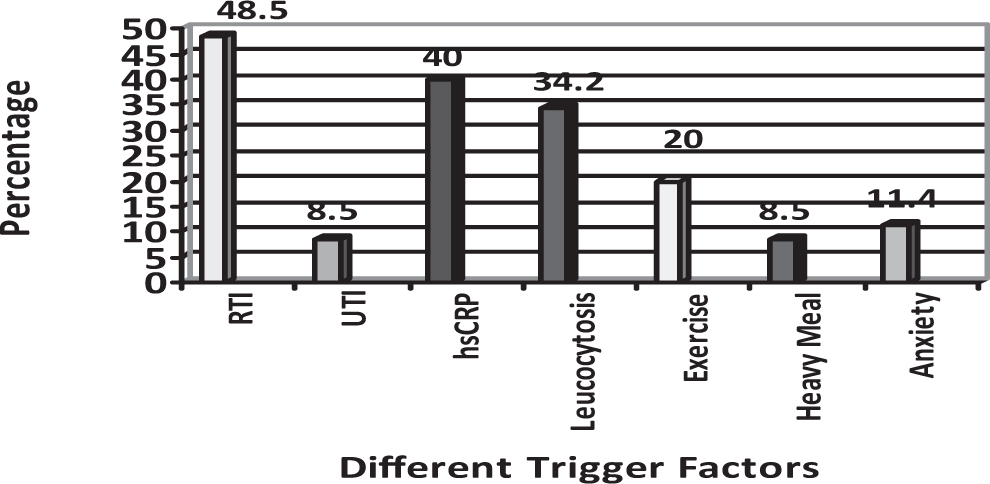
Fig. 1: Percentage of different trigger factors in 70 ischemic stroke patients, studied in Kolkata, India (n =70).
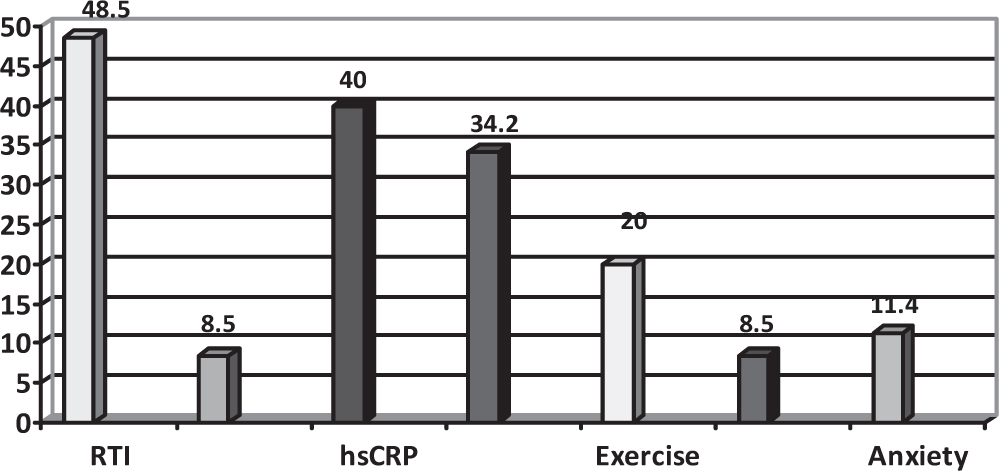
Fig. 2: Percentage of different trigger factors in the control group (n = 80).
Table 4: Demographic features of stroke patients with and without recent infection
| Variable | Infection (n = 40) → 57% |
No infection (n = 30) → 43% |
|---|---|---|
| Age | 63.3 ± 9.42 | 61.4 ± 9.74 |
| Sex (M/F) | 30/10 | 22/8 |
| Smoking | 22 (55%) | 12 (40%) |
| Hypertension | 18 (45%) | 14 (46.6%) |
| Diabetes | 10 (25%) | 8 (26.6%) |
| Dyslipidemia | 16 (40%) | 8 (26.6%) |
| TIA / Prior Stroke | 6 (15%) | 2(6.6%) |
Discussion
Stroke is one of the leading causes of morbidity and mortality all over the world. There are well known chronic risk factors for both blockage of coronary arteries and cerebral arteries. Several earlier studies have evaluated that anger and sexual activity are potential trigger factors in myocardial infarction.3 In epidemiological studies, the leukocyte count has been associated with the risk of myocardial infarction and ischemic stroke.13 A multitude of mechanisms link chronic infection and thrombotic events.14 The most important evidence for the role of chronic infection in atherogenesis but not directly in stroke stems from tissue analysis and not from epidemiological studies. But Koch’s postulates for causality between microbial agent and disease include a specific infection and stroke. Antibodies against CMV, herpes viruses, etc. were associated with (cohort study) carotid intimo-medial thickening.15 Likewise, hepatitis A virus sero-positivity was independently associated with coronary artery disease.16 Viruses including varicella zoster and CMV are also known to cause vasculitic stroke.17
Syrjanen et al17 found that young adults who presented with acute cerebral infarction had higher rates of febrile infection in the preceding month than age/sex matched community control subjects. We studied several trigger factors and found higher prevalence of recent (<2 weeks) infection and inflammation (57%) evaluated clinically by symptoms and signs beside evidence of increased CRP and leucocytosis which are comparable (35%) with the study report of Richard F. Macko et al6 and Syrjanen et al10 (range 28% to 34%). This study also strikingly supports similar results of preceding infection and stroke association done by Grau et al.18
In our present study we have searched for trigger factors in admitted ischemic stroke patients, keeping in mind the previous investigators data and suggestions. As the study area is in the tropical country with poor socio-economic status, infectious diseases are more prevalent than Europe and America, still the different trigger factors are directly or indirectly associated with these stroke patients. Seasonal variation, i.e. more in the fall or winter versus spring and summer (40 versus 30), is consistent with the study of seasonal infection and stroke prevalence done by Hindfelt et al.19 In contrast Macko et al have not found any seasonal variation of infections between stroke group and matched control group. We found that traditional risk factors like smoking, diabetes, hypertension and dyslipidemia have near average prevalence when compared with the control subjects. We also found RTI and UTI as the most common infections in stroke groups which have already been suggested by Macko et al in their study of 37 ischemic stroke patients.6
Though we found 57% of stroke patients were associated with febrile illness and different infections but we got leukocytosis in only 34.2% cases because a few suffer from viral infection and inflammation though leukocytosis, C-reactive protein (CRP) and fibrinogen are independent risk factors in ischemic strokes according to the Grau et al.9 We also found increased CRP levels in 40% of stroke patients as compared to 20% of controlled non-stroke patients indicating that infections and inflammations (evidenced by markers) have strong association with ischemic stroke although ischemic stroke itself can raise the levels of CRP. Another clinical and biochemical assessment regarding CRP levels in ischemic stroke patients was done by us in this study, where we searched for CRP levels between two subgroups i.e., with infections and without infections. We found that 50% of ischemic stroke patients with febrile illness showed higher values of CRP but only 27% of ischemic stroke without infection showed raised CRP values.
From this study it is not obvious that coagulation disorder and atherothrombosis formation are increased with high leukocyte count and CRP. There is one indirect observation of about 70 patients which showed vaccination against common infection (influenza) reduces stroke risk by 50% when compared with community control group.20
Another large CAPRIE (Clopidogrel versus Aspirin in patients at risk of ischemic events) trial showed that short term changes in leukocyte counts result in an increased period of stroke risk.17 In our study, high leukocyte count in 34.2% of stroke patients versus 18% of control group suggests strong association of leukocytosis and coagulation disorder, resulting in increased stroke prevalence. But further study is necessary to investigate the threshold value that can result in stroke or proportionate ratio between neutrophil and ischemic strokes.
Though we couldn’t use negative scale and stressful life events in evaluations of ischemic strokes associated with psychological stress as done by Macko et al and others but we found 20% of stroke patients were in mental stress, state of altercation and depressive mood which is insignificant when compared with the control groups.
We studied two important stroke triggers e.g. heavy exercise (20%) and after heavy meal (8.5%), which are important trigger factors of myocardial infarction as studied earlier by Mitlleman et al.3 Though 20% ischemic stroke cases were associated with heavy exercise but 20% control subjects also had history of heavy exercise (p < 0.5). Like myocardial infarction, association of heavy meal and ischmeic strokes (8.5%) is significantly higher than the control groups (p < 0.003).
From this study and several previous studies it is evident that systemic infections and inflammation are very important trigger factors of ischemic brain strokes. Though in several studies highly sensitive C Reactive Proteins (hsCRP) indicate longstanding low grade inflammation but our retrospective case control study reveals increased levels of hs CRP and leukocytosis in most ischemic strokes with infections (50%) compared to ischemic stroke without infection (27%) and non stroke patients (20%). Though several prospective multicentre trials are necessary for investigating infections, inflammations, leukocytosis and biochemical measurements of hs CRP as trigger factors for ischemic stroke still our preliminary studies indicate early institution of antibiotics and antiplatelets as preventive tools during the period of increased risk of cerebral stroke.
Thus, recognition of the stroke prone state may be helpful for preventive intervention and consequent reduction in incidence of the disease.
The article complies with International committee of Medical Journal Editor’s uniform requirements for the manuscripts.
Competing interests – None, Source of Funding – None
Received Date : 16 December 2010; Revised Date: 06 January 2011
Accepted Date : 23 January 2011
References
1. Donnan GA, Fisher M, Macleod M, et al. Stroke. Lancet 2008; 371: 1612–1623.
2. Sacco RL, Ellenberg JH, Mohr JP, et al. Infarcts of undetermined cause: the NINCDS Stroke Data Bank. Ann Neurol 1989; 25: 382–390.
3. Mittleman MA, Maclure M, Sherwood JB, et al. Triggering of acute myocardial infarction onset by episodes of anger. Determinants of myocardial infarction onset study investigations. Circulation 1995; 92: 1720–1725.
4. Muller JE, Mittleman MA, Maclure M, et al. Triggering myocardial infarction by sexual activity. Low absolute risk and prevention by regular physical exertion. Determinants myocardial infarction onset study investigations. JAMA 1996; 275: 1405–1409.
5. Gurfinkel ET, Fuente RL, Mendiz O, et al. Influenza vaccine pilot study in acute coronary syndromes and planned percutaneous coronary interventions: the FLU Vaccination Acute Coronary Syndrome (FLUVACS) Study. Circulation 2002; 105: 2143–2147.
6. Richard F. Macko, Sebastian F. Ameriso, Robert Barndt, et al. Precipitants of brain infarction. Stroke 1996; 27: 1999–2004.
7. Grau AJ, Buggle F, Heindl S, et al. Recent infection as a risk factor for cerebrovascular ischemia. Stroke 1995; 26: 373–379.
8. Bova IY, Bornstein NM and Korczyn AD. Acute infection as a risk factor for ischemic stroke. Stroke 1996; 27: 2204–2006.
9. Grau AJ, Buggle F, Becher H, et al. Recent bacterial and viral infection is a risk factor for cerebrovascular ischemia. Neurology 1998; 50: 196–203.
10. Syrjanan J, Vattonen VV, Livanainen M, et al. Preceding infection as an important risk factor for ischemic brain infarction in young and middle aged patients. Br Med J 1988; 296: 1156–1160.
11. Varma M. Treatment of acute stroke: recommendations for clinical practitioners. Annals of Neurosciences 2005; 12(2): 27–32.
12. Ridker PM. High-Sensitivity C-Reactive Protein - Potential Adjunct for Global Risk Assessment in the Primary Prevention of Cardiovascular Disease 2001; 103: 1813.
13. Elkind MSV, Sciacca R, Boden-Albala B, et al. Relative elevation in baseline leukocyte count predicts first cerebral infarction, Neurology 2005; 64: 2121–2125.
14. Estein SE, Zhou YF, Zhu J. Infection and atherosclerosis: emerging mechanism paradigms. Circulation 1999; 100: e20–e28.
15. Neito FJ, Adam E, Sorlie P, et al. Cohort study of cytomegalo virus infection as a risk factor for cardio intimal mediate thickening, a measure of subclinical atherosclerosis. Circulation 1996; 94: 922–927.
16. Zhu J, Quyyuni AA, Norman JE, et al. The possible role of hepatitis A virus in the pathogenesis of atherosclerosis. J Infect Dis 2000; 182: 1583–1587.
17. Del Brutto OH. Pathophysiology, Diagnosis and Management. Infectious and stroke. Vol. II Malden, Mass: Blackwell Science 1998; 1639–1640.
18. Grau AJ, Boddy AW, Dukovic DA, et al. Leukocyte count as an independent predictor of recurrent ischemic events. Stroke 2004; 35: 1147–1152.
19. Hindfelt B and Nilsson O. Brain infarction in young adults with particular reference to pathogenesis. Acta Neurol Scand 1977; 55: 145–157.
20. Graw AJ, Fisher B, Barth C, et al. Influenza vaccination is associated with a reduced risk of stroke. Stroke 2005; 36: 1501–1506.
(c) Annals of Neurosciences.All Rights Reserved