Annals of Neurosciences, Vol 16, No 4 (2009)
Nasal paraganglioma with orbital and cranial extension: a rare case report
Corresponding Author
Debabrata Das,MS
E-8 Shyamali Estate,
EA Block, Sector-I,
Salt Lake City,
Kolkata-700064, India.
Tel.: +919433894329
E-mail: debabrata_dr@yahoo.com
ABSTRACT
Paragangliomas are rare neuroendocrine neoplasm of extraadrenal autonomic nervous system. These are usually benign, slowgrowing vascular tumors found in the abdomen, thorax, head and neck region. Head and neck paraganglioma is primarily located in the temporal bone and carotid body. Paragangliomas of nose and paranasal sinuses are rare. Orbital paraganglioma is also extremely uncommon. A nasal paraganglioma with orbital and intracranial extension has not been elaborately reported in the literature. We present here details of such a case.
KEYWORDS: Paragangliomas, nasal, orbital, intracranial extension
doi: 10.5214/ans.0972.7531.2009.160412
Introduction
Paraganglions are a group of chemoreceptor organs widely distributed through out the human body. They originate from neuroectoderm and are composed of type I, chief cells surrounded by supporting type II sustenacular cells.1 These cells are located along blood vessels and are responsible for blood pH changes, regulation of blood pressure and blood flow in the body. 2 Paraganglia have a centripetal and roughly symmetrical distribution in the abdomen, thorax, head and neck.
Paragangliomas are usually benign slow growing vascular neoplasm that arise from the non-chromaffin paraganglionic tissue predominantly found in the abdomen (85%), thorax (12%) and in the head and neck region (3%). 3 The most common sites of this tumor in head and neck region are in carotid body, jugular bulb, along glossopharyngeal and vagus nerves. In about 1-3% of cases, these tumors are malignant. 4 Paragangliomas constitute only 0.012% of all malignancy of human body with estimated annual incidence as one case per 1.3 million people. 1,5These tumors occur more frequently in women with a female to male ratio 4:1 in 5th to 6th decade of life. 6 Paraganglioma of nose and paranasal sinuses are very rare. ' Orbital paragangliomas are also extremely uncommon.2,3, 7We report here a case a nasal paraganglioma with orbital and intracranial extension.
Case Report
A 35-year-old woman presented to us with complaints of epistaxis, nasal obstruction, proptosis of the left eye and a forehead swelling for 6 months. She had no preceding history of trauma. Past history was nothing significant. On clinical examination, a well-defined firm, 5cm in diameter, immovable mass with bruit was found in her left side of forehead. Surrounding frontal bone defect was also detected on palpation of the swelling. Rhinoscopy showed a polypoid mass in the left nasal fossa obstructing ipsilateral coanal area with blood stained secretion. Ophthalmological examination revealed mild hypotropia and exotropia of the left eye with 8mm inferotemporal proptosis that was not compressible or reducible. Visual acuity was 20/20 in right eye and 20/60 in left eye. Pupils were equal and reactive to light. Corneal reflexes were present. Fundus examination revealed no abnormality. She had no cervical lymphadenopathy. Her blood pressure was 130/86 mm of Hg with regular 76/min pulse rate. Hematological and serum biochemistry tests were normal.
Computed tomography (CT) scan showed a well-defined soft tissue density lesion in the left nasal cavity, left orbit left subfrontal area with erosion of bony wall of frontal sinus and part of left frontal lobe at medial aspect. Contrast study showed homogenous enhancement. Magnetic resonance imaging (MRI) of brain showed a large (88mmX55mmX53mm) hetero-geneously enhancing mass with variable T1 8 &T2 lengthening in the left frontal sinus, left subfrontal area, orbit and left ethmoidal sinus (Figure 1). MRI also showed osteolytic lesion in the left side of frontal bone. T1-weighted images showed typical isointense with serpiginous flow void areas with 'salt and pepper' appearance of the tumor matrix. The FNAC of left nasal cavity tumor mass showed polygonal cell nests surrounded by fibrous tissue that was suggestive of paraganglioma.
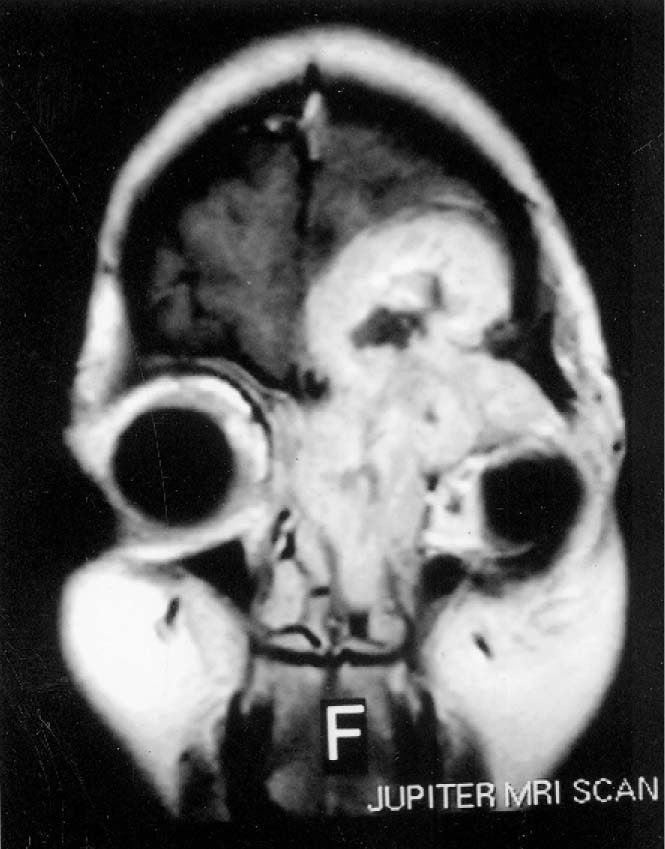
Fig. 1 :: MRI showing a mass in the left nasal cavity, left orbit and involving left frontal lobe.
After discussion with otolaryngologist, a multidisciplinary team approach was taken for surgical removal of the paraganglioma. It was planned through fronto-orbito-rhinotomy approach to excise intranasal, intraorbital and frontal tumor mass. The intracranial tumor mass was completely removed and repair of the frontal bone defect was done by cranioplasty with methyl methacrilate following sealing of dural defect with durograft and fibrin glue. The nasal mass was also completely removed. The orbital mass was incompletely excised due to close association with the optic nerve. No immediate postoperative complication was observed. Histological section of the tissue showed large polygonal to oval cells arranged in chemodectomatous and nesting pattern, surrounded by a delicate fibrovascular stroma forming characteristic Zellbellan pattern (Figure 2). The cells had abundant eosinophilic cytoplasm and round nucleus with mild pleomorphism. These features confirmed diagnosis of paraganglioma.
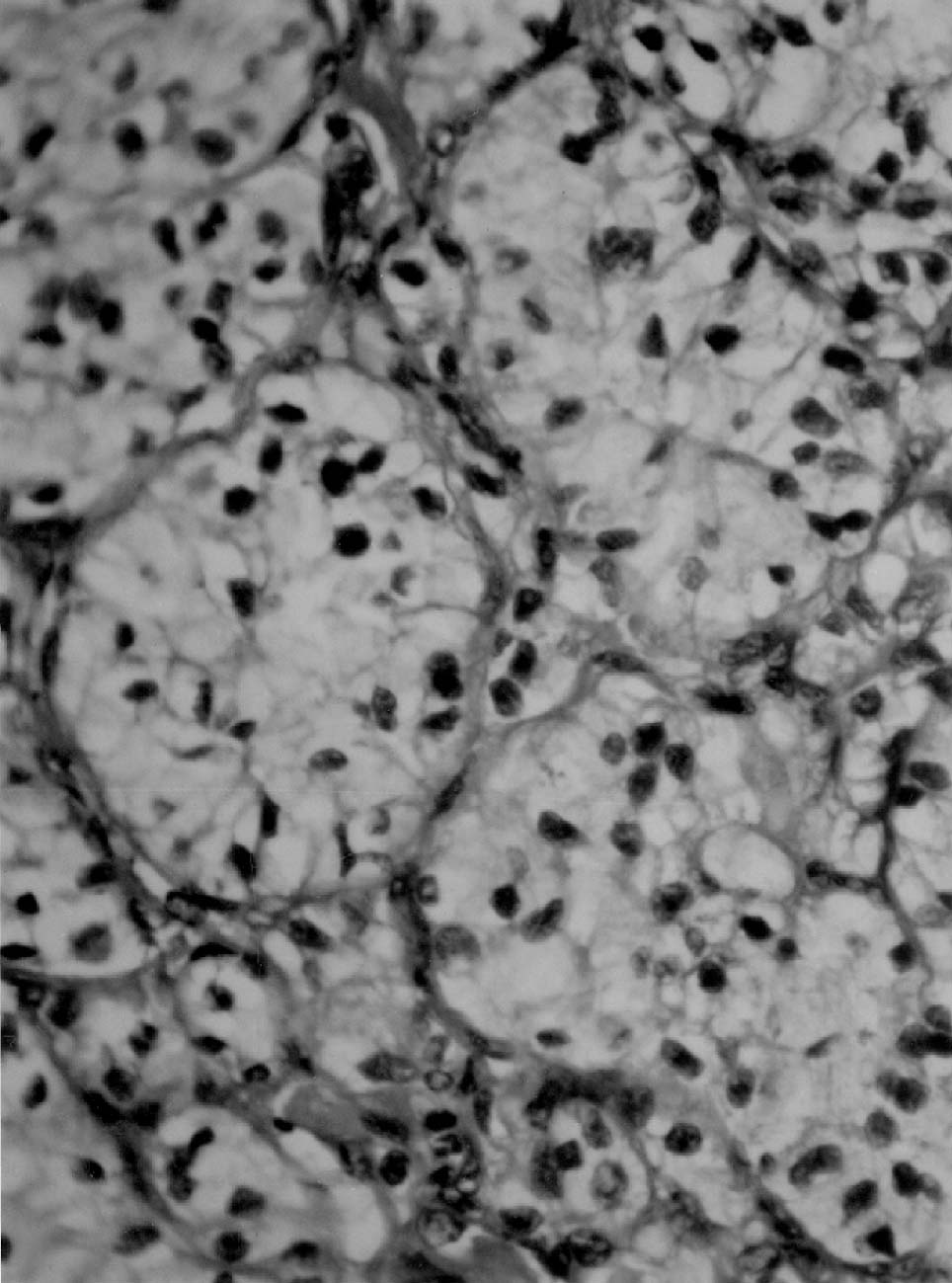
Fig. 2 :Histopathology of the excised tissue showing nests of epitheloid cells in 'zellballen' pattern, characteristic of paraganglioma (Hematoxylin and eosin stain; original magnification x400).
Her proptosis reduced and visual acuity improved to 20/30 in the left eye after 3 weeks. She was advised to repeat MRI of brain, orbit and paranasal sinuses. However, the patient lost to follow up.
Discussion
Paragangliomas are usually benign, slow growing tumors and rarely become malignant. Multiple site involvement of the tumor may occur in 10 - 20% patients with positive family history as a part of multiple endocrine neoplasias.4
The exact site of origin of nasal and paranasal sinuses paragangliomas is still unknown. Some authors suggested of sustenticular origin whereas others thought of ciliary paraganglionic origin.7 In our case, the tumor arose from the lateral nasal wall and extended to the orbit and cranium with involvement of the left frontal lobe. Because of local aggressive behavior of the tumor, frontal bone was eroded. The tumor extended into the left orbit to cause proptosis.
As paragangliomas progressively invade local vital structures, surgical excisions including disease free zone remain the treatment of choice for these tumors. 2 Therefore, a multidisciplinary team approach was taken for surgical removal of the paraganglioma through fronto-orbito-rhinotomy approach with excision of the forehead mass. Anand et al 9 reported about difficulty in distinguishing intracranial paraganglioma from normal tissue and suggested to leave residual tumor mass to avoid surrounding tissue damage. In our case, the forehead mass with intracranial extension and the nasal mass were completely removed. The orbital mass was incompletely resected due to close association with the optic nerve. Some authors have suggested full dose radiation therapy (4500-6000 rad) for the residual tumor mass though results are variable. 1 Therefore, we planned radiation therapy for the residual tumor mass. After 3 weeks of follow up, she was advised to repeat M RI of brain, orbit and paranasal sinuses. However, the patient was lost to follow up subsequently. After extensive MEDLINE search, we could not find a case of nasal paraganglioma having orbital and intracranial extension with bone erosion.
In conclusion, this case has been presented to highlight the local extension of nasal paraganglioma that required a multidisciplinary team approach.
Competing interests - None, Source of Funding - None
Received Date : 16 July 2009; Revised Date : 28 August 2009
Accepted Date : 16 September 2009
References
1 Nguyen QA, Gibbs PM, Rice DH. Malignant nasal paraganglioma. Otolaryngol Head NeckSurg 1995; 113:157-61.
2 Jothi M, Keshava R, Gope ML, et al Possible role of the tumor suppressor gene retinoblastoma (rbi) in human brain tumor development. Annals of N eu rosei enees 2 007; 14(3) 7 2-82.
3 Bednar MM, Trainer TD, Aitken PA. Orbital paraganglioma: case report and review of the literature.Br J Ophthal 1992; 76:183-85.
4 Zak FG, Lawson W. The Paraganglionic Chemo receptor System: Physiology, Pathology And Clinical Medicine New York, Springer-Verlag, 1982.
5 Mertens WC, Grignon DJ,Romano W. Malignant paraganglioma with skeletal metastases and spinal cord compression: Response and pallation with chemotherapy.Clin Oncol(R Coll Radiol) 1993; 5:126-28.
6 Wasserman PG, Savargaonkar P. Paragangliomas: Classification, pathology, and differential diagnosis. Otolaryngol Clin North Am 2001;34:845-62.
7 Sharma MC, Epari S, Gaikwad S, et al Orbital paraganglioma: report of a rare case. Can J Ophthalmol 2005; 40:640-44.
8 Archer KF, Hurwitz JJ, Balogh JM, et al Orbital nonchromaffin paraganglioma. A case report and review of the literature. Ophthalmology 1989; 96:1659-66.
9 Anand VK, Leonetti JP, Mefty O. Neurovascular considerations in surgery of glomus tumors with intracranial extension. Laryngoscope 1993; 103:722-28.
(c) Annals of Neurosciences.All Rights Reserved